 |
 |
||
|---|---|---|---|

Informed Consent:
Dr. Nowzaradan is a leader in the performance of surgical techniques laparoscopically. Today, surgeries of all types, not just bariatric, are performed using this less invasive technique. Dr. Nowzaradan has published numerous papers on laparoscopy. Prior to his accomplishments, many within the medical community thought his theories of laparoscopically performing various open procedures was impossible. Today, 15 years later, they are commonplace.
|
Restrictive Function Also called the Vertical Sleeve Gastrectomy, the Gastric Sleeve is a restrictive form ofbariatric (weight loss) procedure. As with both the Lap Band System and the Roux-en Y Gastric Bypass, the Vertical Sleeve Gastrectomy utilizes a restrictive function. This means that there is a component to the surgery that restricts the amount of food that a patient needs in order to feel full, decreasing the likelihood of overeating. |
|||
| Laparoscopic Technique As with most weight loss surgeries, the Vertical Sleeve Gastrectomy is typically performed laparoscopically. Instead of making long incisions and literally "opening" a patient, Dr. Nowzaradan makes a series of small incisions (about ½ inch to 1 inch in length) in the abdomen. At least one of these incisions is used to insert a temporary device, called a trocar, which allows the doctor to introduce carbon dioxide gas into the abdomen, inflating it, thereby creating a larger workspace in the abdominal cavity. A tiny camera is inserted through one of the remaining small incisions. This sends a live, clear picture to a monitor in the operating room, which Dr. Nowzaradan uses to visually guide delicate surgical instruments within the patient's abdomen. These instruments are inserted through the final remaining incision(s). Once the procedure is complete, the excess abdominal gas is expelled, the trocars removed, and the incisions are closed. |
Advantages of Laparoscopic Technique Obese and morbidly obese patients who undergo a laparoscopic approach do better overall in their recovery when compared to patients who undergo an open procedure and experience large incisions. Laparoscopic procedures cause far less physical trauma to a patient than do open procedures, they are less invasive, result in more rapid healing and recovery times, and cause minimal scarring. |
|||
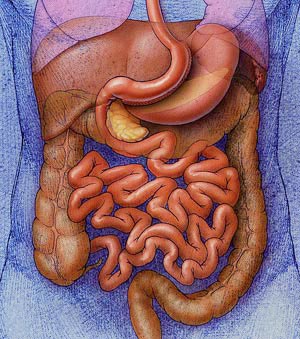
| Anatomy of the Vertical Sleeve Gastrectomy The Gastric Sleeve uses a surgical stapling technique to seal off and remove part of the stomach. Because the decommissioned portion of the stomach is removed, the procedure is not reversible. The remaining functional portion of the stomach is larger than that created with a Roux-en Y Gastric Bypass procedure. With the Gastric Sleeve, about 85% of the stomach is removed. The remaining, smaller stomach pouch follows the original major curve, creating a sleeve-shape with a volume of 30cc to 150cc; about the size of a small banana. Relative Similarity to Pre-surgical Digestive System In an unaltered digestive system, food enters the stomach and is partially broken down by digestive juices into a product called "chyme". The pylorus, or pyloric sphincter or valve, regulates the passage of chyme from the stomach into the upper part of the small intestine (the duodenum). It usually takes somewhere between 40 minutes to a few hours for the stomach to digest food. Chyme then slowly passes into the duodenum through the pyloric valve. |
By comparison, with the Roux-en Y Gastric Bypass procedure, a greater portion of the stomach is divided off and decommissioned, including the part that contains the pylorus. With a Roux-en Y, a new stomach exit into the small intestine is created. The retaining or removal of the pylorus from the digestive tract creates unique advantages and disadvantages to each of the procedures.
|
|||
| Relatively Few Post-surgical Food Restrictions Because wth the Gastric Sleeve, the new stomach pouch is essentially a smaller version of the original organ, there are fewer restrictions to the types of food that a patient can eat post-operatively than with some other bariatric procedures. In addition, the removal of this large amount of stomach, and especially the specific area of the stomach that is removed, significantly decreases the amount of hunger-producing hormones that the stomach can continue to introduce into the patient's system. Overall Decrease in Hunger and Cravings |
Also, with the Gastric Sleeve, the removed section of the stomach is actually the portion that stretches the most. The long vertical tube-shaped stomach that remains is the portion least likely to expand over time. It creates significant resistance to higher volumes of food. The physics of retaining a sleeve-shaped portion of stomach are beneficial as well. Resistance is greatest the smaller the diameter and the longer the channel. Not only is appetite reduced, but also very small amounts of food generate early and lasting satiety (fullness).
Regular Nutrient and Calorie Absorption |
|||
| Personal Suitability for Vertical Sleeve Gasrtrectomy For instance, a Gastric Sleeve may be a more appropriate form of weight loss surgery for patients who are already suffering from anemia, Crohn’s disease, or a variety of other conditions that would place them at high risk for surgery involving malabsorption. The Gastric Sleeve is also the procedure deemed most appropriate for individuals who are classified as super-obese (BMI of 60 or greater – see What is Obesity? page in the Obesity Fact s section of our website). In such instances, the Vertical Sleeve Gastrectomy is often performed as the first stage of a two-stage bariatric strategy. Once the Gastric Sleeve is performed and the patient has experienced sufficient weight loss, the initial procedure may be followed by one involving intestinal bypass. It is also one of the very few procedures that can be performed on the super-obese laparoscopically. |
Disadvantages A common disadvantage of the Gastric Sleeve procedure is that it frequently does not produce the desired amount of weight loss. Patients who undergo a Vertical Sleeve Gatsrectomy may even experience weight regain, because the smaller stomach with its regular function intact, has the potential to grow back in size. This disadvantage, while true of any purely restrictive type of procedure, seems especially problematic with the Gastric Sleeve. Post-surgical Complications |
|||

| Forward to Revisions Page of "Surgical Treatments" Section |