 |
 |
||
|---|---|---|---|

| Roux-en Y, Weight Loss and Post-operative Care The Roux-en Y Gastric Bypass (RNYGB) procedure is in many ways today’s preferred bariatric (weight loss) procedure because it is somewhat more predictable than many other procedures and typically produces greater weight loss and better long-term results, especially when post-operative care and behavior modification is followed. |
Make no mistake though; once a patient has undergone a Roux-en Y Gastric Bypass, inconvenience, discomfort and complications are common if he or she does not alter their dietary habits significantly. The RNYGB can produce significant long-term weight loss results. Depending on a patient’s pre-surgical weight, weight loss of 80 to 140 pounds is common, or 50% - 80% of excess weight. |
|||
Informed Consent: |
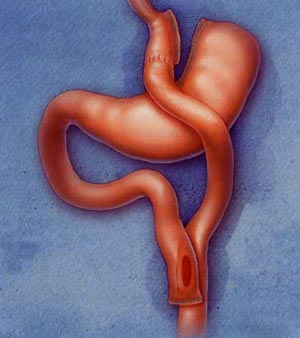
Anatomy of the Roux-en Y Gastric Bypass The Roux-en Y Gastric Bypass changes the anatomy of the digestive system in ways that neither the Lap Band System nor the Vertical Sleeve Gastrectomy does. The RNYGB is a procedure that utilizes both a restrictive and malabsorptive function to help a patient lose weight and keep weight off. Restrictive Function Malabsorptive Function |
 |
||
|
Laparoscopic Technique As with most weight loss surgeries, the Roux-en Y Gastric Bypass is typically performed laparoscopically. Instead of making long incisions and literally "opening" a patient, Dr. Nowzaradan makes a series of small incisions (about ½ inch to 1 inch in length) in the abdomen. At least one of these incisions is used to insert a temporary device, called a trocar, which allows Dr. Nowzaradan to introduce carbon dioxide gas into the abdomen, inflating it, thereby creating a larger workspace in the abdominal cavity. A tiny camera is inserted through one of the remaining small incisions. This sends a live, clear picture to a monitor in the operating room, which Dr. Nowzaradan uses to visually guide delicate surgical instruments within the patient’s abdomen. These instruments are inserted through the final remaining incision(s). Once the procedure is complete, the excess abdominal gas is expelled, the trocars removed, and the incisions are closed. |
Obese and morbidly obese patients who undergo a laparoscopic approach do better overall in their recovery when compared to patients who undergo an open procedure and experience large incisions. Laparoscopic procedures cause far less physical trauma to a patient than do open procedures, they are less invasive, result in more rapid healing and recovery times, and cause minimal scarring.
Dr. Nowzaradan and Laparoscopic Pioneering |
||
 |
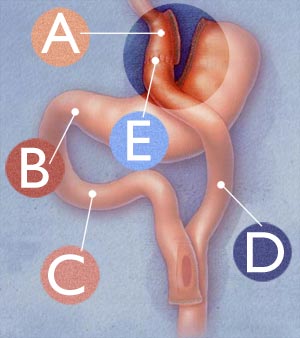
RNYGB Procedure The Roux-en Y Gastric Bypass procedure begins with the restrictive component. Dr. Nowzaradan sections off the majority of the stomach reservoir, creating a substantially smaller stomach pouch where the esophagus meets the stomach (called the esophago-gastric junction). The larger, disconnected portion of the original stomach is removed from primary involvement in the digestive tract. Specially designed surgical staples are used to seal the sectioned components. Thi sis illustrated at A below.
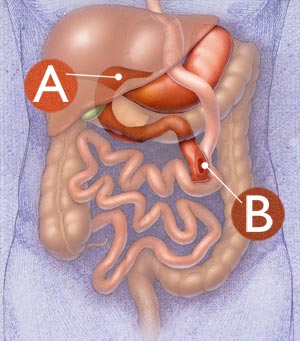
Only the uppermost part of the stomach, that part which is directly at the esophago-gastric junction, remains part of the primary, newly designed digestive tract. This remaining stomach pouch size is about 1 ounce, or the size of a golf ball. This pouch cannot hold much volume of food, which causes the patient to feel fuller sooner. In addition to this restrictive element is the malabsorptive function. Normally, the stomach empties directly into the small intestine through the pyloric valve (identified at B above). The upper part of the small intestine, which the stomach would normally empty into first, is called the duodenum (doo-oh-DEE-num), identified at C above. The lower part of the small intestine is called the jejunum (jay-JOO-num), D above). With the RNYGB, Dr. Nowzaradan sections off these two parts of the small intestine, bypassing the duodenum, and connects the new, smaller smooch pouch directly to the lower part of the small intestine, the jejunum. This connection is illustrated at E above. Significance of Duodenal Bypass In addition, the duodenum absorbs fat. With its removal from primary digestive function, the body absorbs less fat. |
Further, the duodenum is the portion of the small intestine that produces and distributes bile, pancreatic acids and other secretions that facilitate the complete breakdown of food into its constituent parts. Again, by removal the duodenum from primary function, food is not broken down as effectively as in an unaltered digestive system; thereby allowing less absorption of calories.
Secondary Function of the Stomach
Procedure Duration The Roux-en Y Gastric Bypass is in fact a reversible procedure, because all the original parts of the digestive tract remain intact, healthy and available within the patient’s abdomen; however, reversals are a form of revision surgery and are far more complicated and unpredictable than the original procedure. Do not select a Roux-en Y Gastric Bypass based on its theoretical reversibility. |
||
| Recommended Post-operative Behavior Modification While this procedure is typically very effective for weight loss, the significant anatomical alterations make it necessary for you to make fundamental changes to your post-surgical eating habits or face discomfort and complications. RNYGB's require adherence to proper post-surgical diet not only to maintain optimum long-term weight loss effects, but also to compensate for the medical conditions that precipitate from the removal of portions of the natural digestive tract. Dumping Syndrome Dumping Syndrome occurs because of the surgical alteration of the motor functions of the stomach. When most of the original stomach was sectioned off and decommissioned from primary function in the digestive system, so was the pylorus, or pyloric valve. In an unaltered system, this valve serves as the stomach’s natural exit into the duodenum and regulates the passage of partially digested food into the small intestine. Without the pylorus, under certain conditions, this passage is uncontrolled. Dumping Syndrome can occur in 2 stages. The early stage symptoms occur 15-60 minutes after eating. Early stage is caused when sugar and simple carbohydrates pass too rapidly into the small intestine. The body's response is to pull fluid into the small intestine, resulting in bloating, abdominal pain, diarrhea and shortness of breath. Late stage symptoms occur anywhere form 1-3 hours after eating and may include weakness, sweating, anxiety, dizziness or even fainting. |
To avoid Dumping Syndrome and slow the rate of emptying, drink liquids sparingly and slowly during meals. A post-RNYGB diet should be high in protein and low in carbohydrates and simple sugars. Refer to the Nutritional Guidance page of the Outreach section of our website to learn about sources for these food components. Because of the alterations to the anatomy of the digestive system, a post-RNYGB diet should not follow the same proportion guidelines as suggested on the Nutritional Guidance page, but you should certainly maximize the nutrient potential of the foods you choose to eat.
Dietary Behavior Post-RNYGB Also, because of the malabsorptive nature of this procedure, vitamin and mineral supplements must be taken post-operatively for life. Post-surgical Complications and Side Effects Post-surgical side effects may include: hair loss, fatigue, dry skin, chills, body aches, mood changes, vitamin deficiency, dehydration, gallstones, stomach ulcers, intolerance to certain foods, kidney stones, and low blood sugar. |
|||
| Forward to Lap Band System Page of "Surgical Treatments" Section |